The clear aligner industry has grown at an unprecedented pace. As market leaders race to expand across multiple regions, a critical question keeps surfacing:
How do you scale clear aligner design without sacrificing clinical quality
Two very different answers have emerged. The first — adopted by most ultra-large brands — fragments the design process into 5–8 separate stages. The second gives a single designer complete ownership of the entire treatment plan, supported by AI.
The difference in outcomes? It’s bigger than most people realize.
The Assembly-Line Model: Built for Scale, Not for Quality
To support multi-regional design centers, many leading clear aligner brands break the design workflow into hyper-specialized stages. One designer handles segmentation. Another places attachments. A third manages staging. Each person owns just one or two steps.
The logic seems sound: designers are easier to replace, training is faster, and quality checkpoints can be added at each stage. Workforce stability improves because designers must stay for years to learn the full process.

But uncover the surface, this model creates problems that no amount of process optimization can fix.
The Hidden Costs of Fragmentation
No One Sees the Full Picture
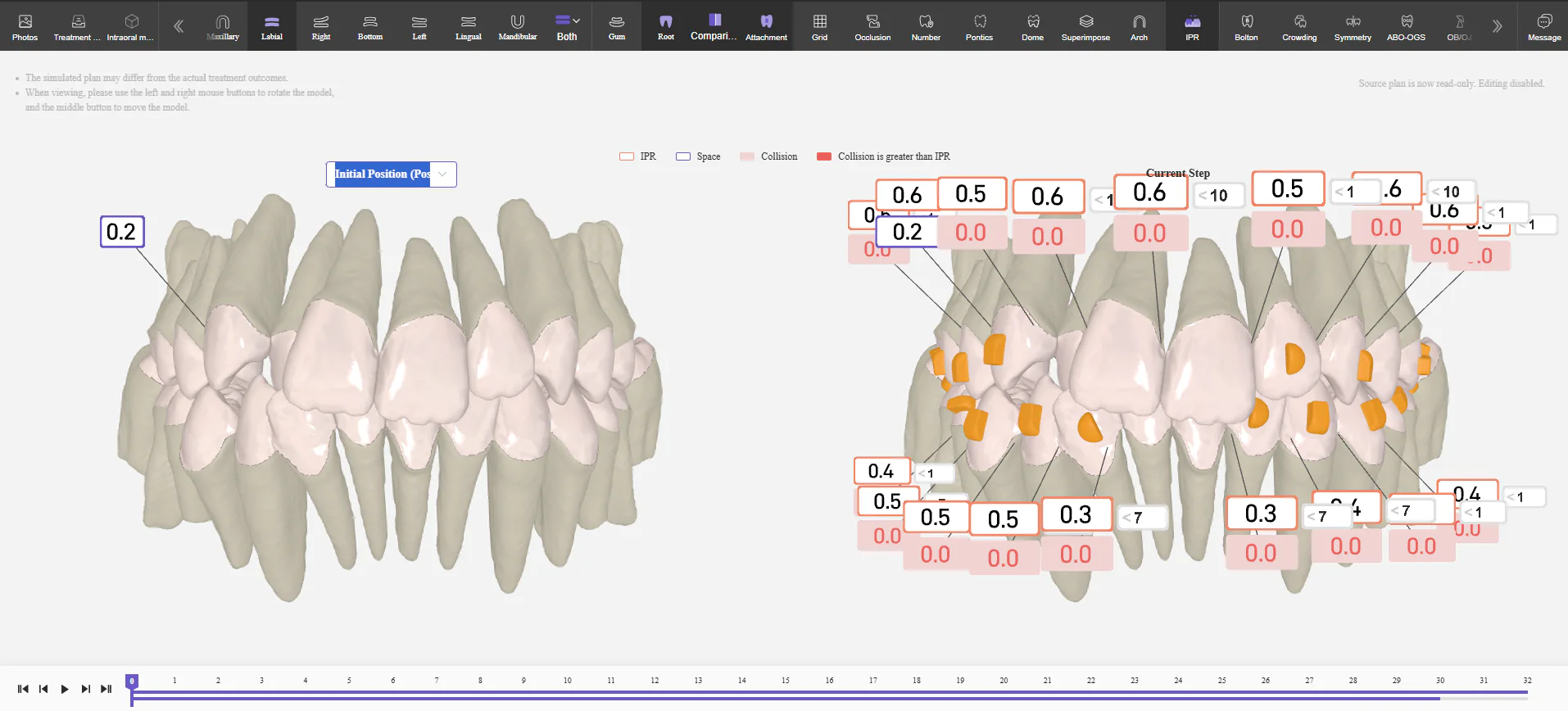
In clear aligner treatment planning, every decision is connected. Attachment placement affects staging. Staging affects interproximal reduction. IPR affects the final occlusion. When five different people make these decisions in isolation, the plan loses its internal coherence.
Each stage may look correct on its own. But when you put them together? The result often fails to achieve the desired clinical outcome — especially in moderate and complex cases.
Refinement Rates Stay High
When the plan lacks coherence, patients don’t track as predicted. Mid-course corrections pile up. Treatment times extend. Refinements and restarts become the norm rather than the exception — driving costs up and patient satisfaction down.
Communication Breaks Down
When a dentist calls with a question about a treatment plan, no single person can explain the full clinical rationale. Customer service has to trace the case across multiple departments, piecing together fragmented answers.
The treatment plan becomes a “black box” — opaque, difficult to explain, and hard to defend.
The Full-Process Model: One Designer, One Vision
The alternative is elegantly simple: one designer owns the entire treatment plan from initial assessment through final staging. Every decision is made within a unified clinical framework.
The catch? This model demands more from designers. They need deep knowledge of clinical orthodontics, biomechanics, and software tools. The barrier to entry is higher — but so is the quality of the output.
AI: The Force Multiplier
If the full-process model depends on elite designers, how do you scale it? The answer is AI — specifically, purpose-built AI clear aligner design software.
Best Smile Tech’s AI-native platform amplifies what a skilled designer can do. Routine computational tasks are automated. Intelligent recommendations for attachment placement and staging are grounded in a massive database of proven clinical outcomes. The designer stays in full control — making every final decision — while the software handles the repetitive technical work.
One-designer-per-case, amplified by AI, delivered through a cloud platform with 48-hour turnaround. That’s the new paradigm.

The Human Factor
AI doesn’t replace the designer — it amplifies them. The full-process model still depends on people with strong clinical knowledge and educational foundations.
This shifts how scaling works. Instead of making designers interchangeable, you invest in making them exceptional. The quality of your local designer pool directly determines the quality of your treatment plans.
Geographic expansion requires thoughtful talent development — not just process replication. Organizations that embrace this build lasting advantages: stronger outcomes, deeper provider trust, lower long-term costs, and a reputation rooted in real quality.
The Bottom Line
The assembly-line model enabled rapid geographic expansion, but its limitations are now clear: fragmented clinical thinking, high refinement rates, broken communication, and plans that are technically correct yet clinically incoherent.
The full-process model, powered by AI trained on 100,000+ CBCT-integrated cases, offers a better path. It puts clinical ownership where it belongs — in the hands of skilled designers — and amplifies their capabilities with intelligent automation.