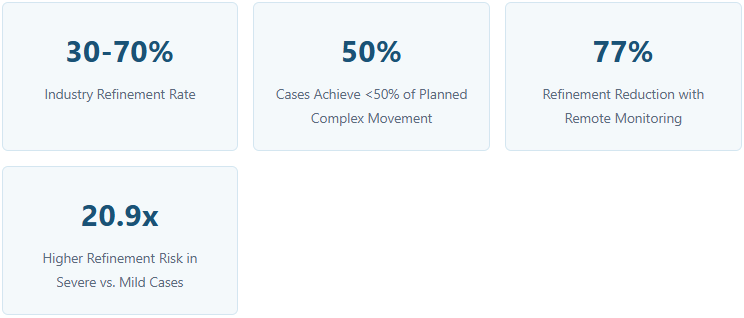
Clear aligner refinements affect 30-70% of cases industry-wide. While mild crowding cases often sail through untouched, moderate and complex cases routinely require multiple refinement cycles. Understanding what drives refinements — and applying targeted prevention strategies — is essential for predictable outcomes and practice efficiency.
What Are Refinements?
Refinements are additional aligner sets prescribed when the initial sequence fails to achieve planned tooth positions. They reflect the gap between digital prediction and biological reality. While not inherently a clinical failure, excessive refinement rates signal room for improvement in planning, technique, or patient management.
![]()
Top Causes of Clear Aligner Refinements
1. Low-Predictability Tooth Movements
Research classifies tooth movements by their expression accuracy. The lowest predictability movements are the biggest refinement drivers:
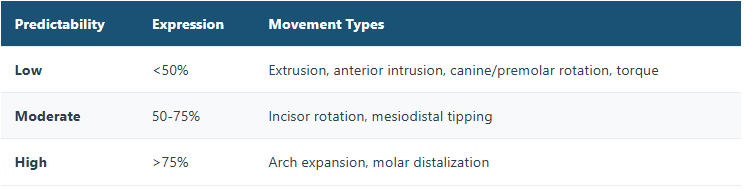
Canine and premolar rotations are particularly problematic — accuracy drops to just 36-40% due to cylindrical root morphology. Vertical movements fare even worse: anterior extrusion achieves only ~30% of planned movement, while intrusion reaches ~41%. Torque control remains a biomechanical challenge, with maxillary incisor torque imprecision ranging from 0.5° to 8.5°.
2. Patient Non-Compliance
Insufficient wear time is the single most common and most preventable cause of tracking failure. Patients wearing aligners fewer than 16 hours daily achieve only 40-50% success versus 85-90% for compliant wearers (20-22 hours/day). The first 6-week checkup is the critical window to catch and correct compliance issues.
3. Planning Errors
Overly aggressive movement velocities, improper staging of rotations/extrusions, and treating complexity beyond the aligner’s biomechanical envelope all cause predictable failure. Key per-tray limits: canine/premolar rotation <1.5°, anterior extrusion <0.25mm.
Why Moderate & Complex Cases Suffer Most
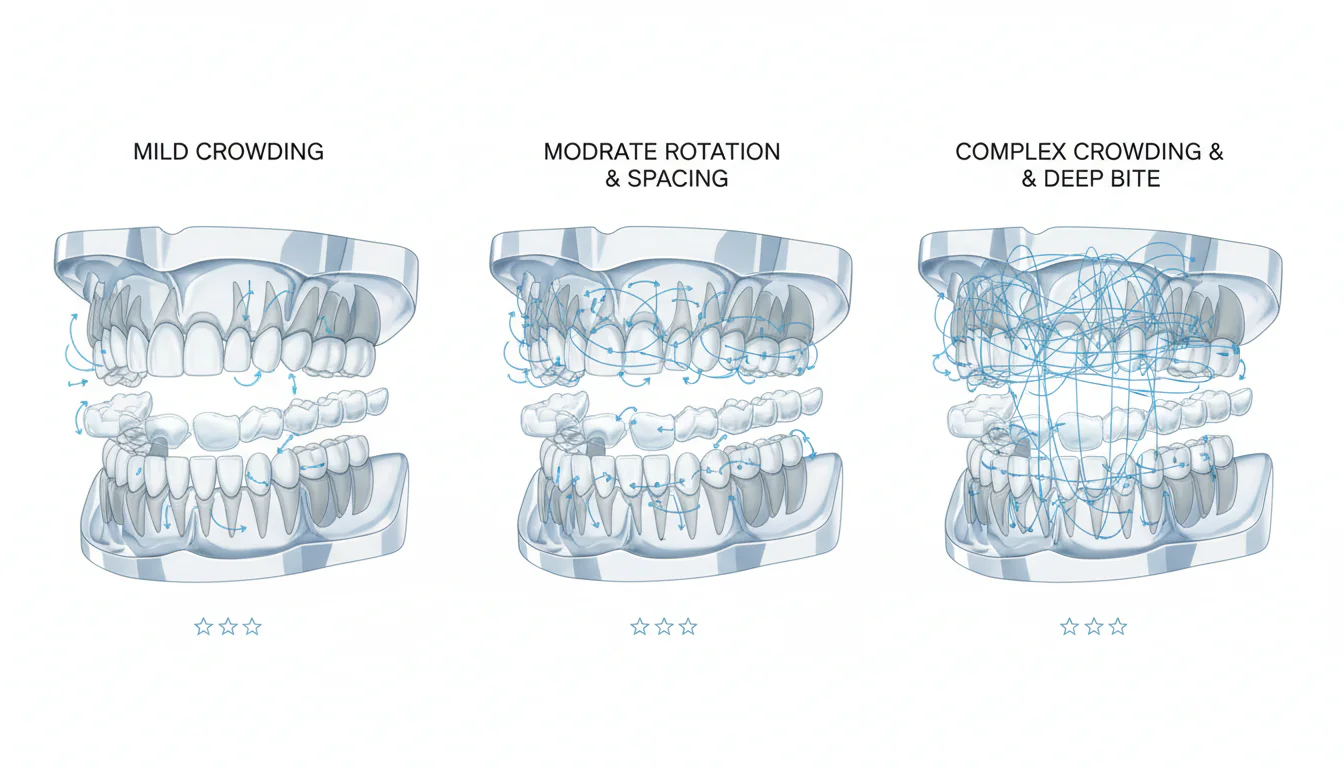
Refinement risk is not linear — it is exponential with complexity:
Mild cases (1-3mm crowding): Often complete with zero refinements; 90%+ initial success.
Moderate cases (4-5mm crowding, 10-20° rotations): Typically require 1-2 refinements.
Complex cases (severe rotations >20°, deep bites <50%, extraction therapy): Frequently need 3+ refinements. Severe spacing cases carry a 20.9x higher refinement probability than mild cases.
The compound effect is the killer: complex cases don’t just have one difficult movement — they demand multiple low-predictability movements simultaneously (torque + vertical control + rotation + space closure), creating multiplicative rather than additive uncertainty.
Deep Bite Reality Check
ClinCheck software overpredicts overbite reduction in 87-97% of cases. Patients achieve only 43-55% of planned overbite opening. The deeper the pretreatment overbite, the greater the discrepancy.
Proven Strategies to Reduce Refinements
1. Rigorous 3D Planning
Treat the virtual setup as a workspace, not a preview. Implement 2-3 iterative review cycles between clinician and lab. For complex cases, integrate CBCT to visualize root positions relative to cortical plates. Adhere to conservative per-tray movement limits — never let software defaults override clinical judgment.
2. Strategic Overcorrection
Build 20-30% overcorrection into the digital setup for movements that predictably under-express:
Canine/premolar rotations: 20-30%
Anterior extrusions: 25-30%
Deep bite correction: up to 150% supercorrection for severe cases
3. Optimize Attachments
Attachments are not optional — they are biomechanical necessities. Select attachment types based on the specific movement: horizontal for rotations, optimized extrusion attachments for vertical movement, vertical rectangular for root uprighting. Ensure adequate clinical crown height for attachment retention.
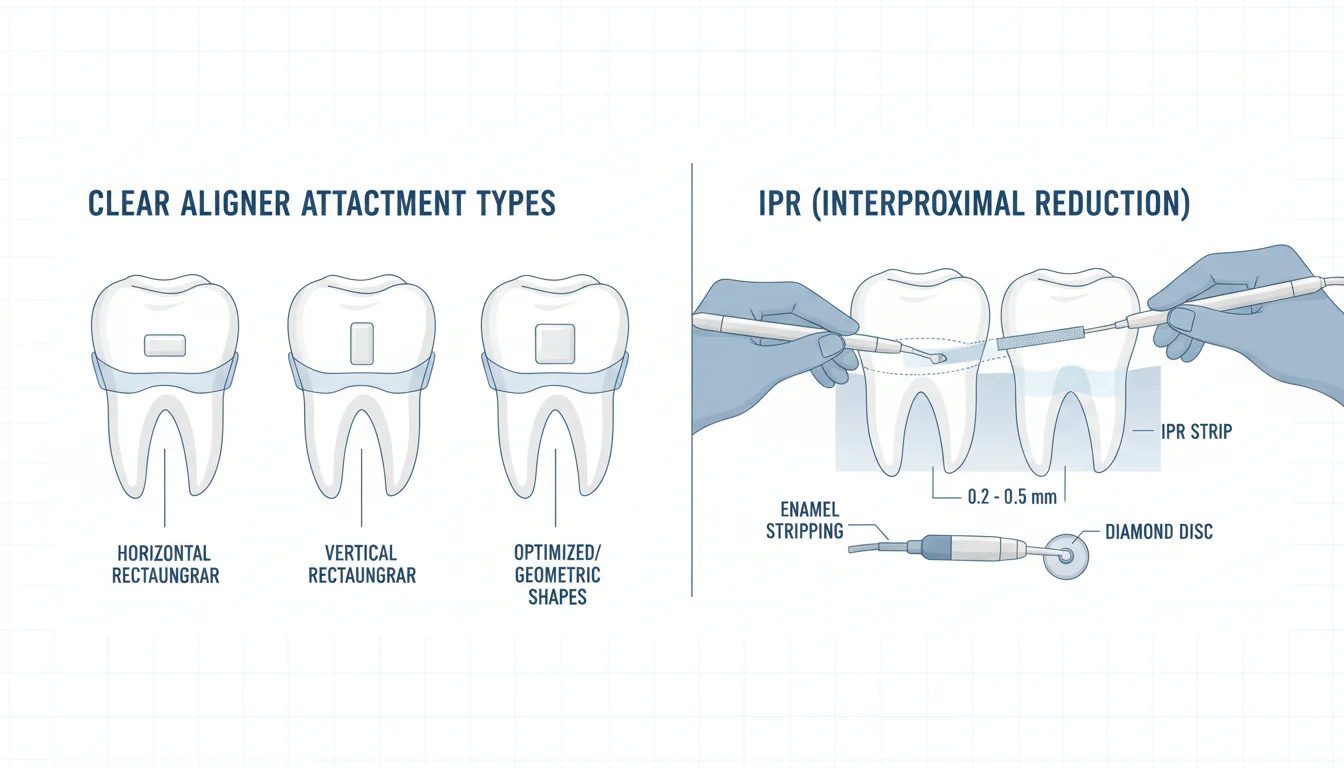
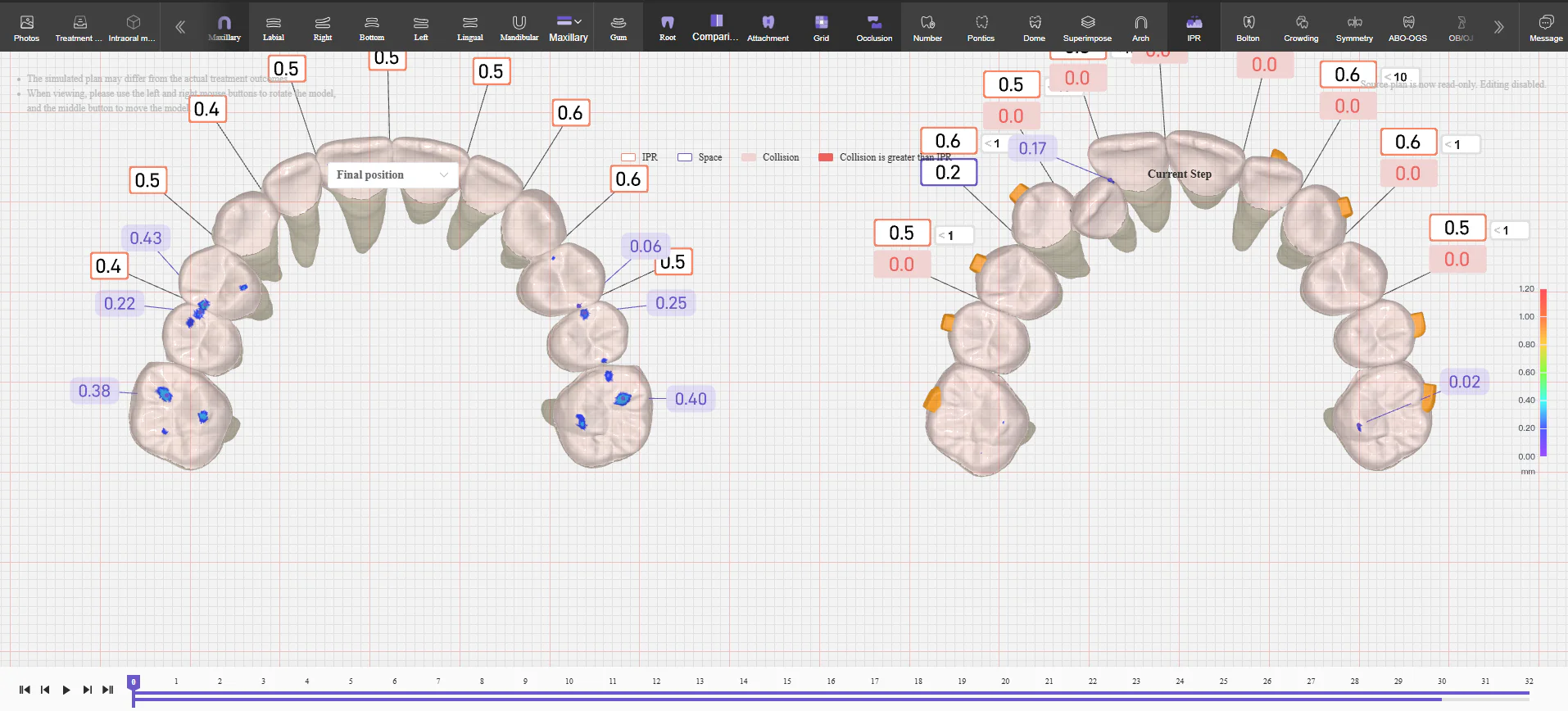
4. Precise IPR Execution
IPR accuracy is only 49% in the upper arch and 42% in the lower arch. Verify planned reduction with gauges — never rely solely on software estimates. Perform incrementally (max 0.3mm per contact), polish all reduced surfaces, and synchronize IPR timing with the alignment that needs it.
5. Sequential Staging
Don’t attempt everything simultaneously. Use phased staging: (1) leveling and aligning, (2) space management, (3) detailed finishing. This gives each movement type room to express before the next biomechanical demand begins.
6. Lock in Compliance
• Set the 22-hour expectation before treatment starts and explain why
• Use color-changing compliance indicators for objective wear-time assessment
• Assess compliance at the 6-week checkup — catch issues before they cascade
7. Proactive Monitoring

The fastest way to reduce full refinements is to catch tracking failures while they are still small enough to correct without a complete case rescan and replan. Implementing systematic monitoring creates this early intervention window:
The 6-Week Checkpoint
By tray 4-6, any significant tracking loss becomes visible through gaps between tooth and aligner, unexpressed rotations, or missed attachment engagement. A structured review at this stage enables corrective intervention: extending wear time on the current tray, adding a chairside button or composite, or backing up one stage to recover engagement.
Remote Monitoring Platforms
Photo-based remote monitoring has matured into a reliable early warning system. Studies demonstrate that DentalMonitoring integration with clear aligner treatment results in a 77% decrease in the number of refinements, 70% reduction in doctor appointment time, and 39% decrease in overall treatment length compared to non-monitored cases. AI-powered analysis flags tracking deviations before they would be caught in person, and the data trail supports cleaner refinement decisions when one is genuinely needed.
8. Leverage Adjunctive Technologies
For moderate and complex cases, several adjunctive technologies can improve movement predictability:
Red light therapy (photobiomodulation): Low-level red and near-infrared light stimulates osteoclast and osteoblast activity, accelerating bone remodeling. Clinical studies show it increases the rate of tooth movement, reduces patient discomfort, and improves expression of challenging movements. Practices incorporating red light therapy report shorter aligner change intervals and significant refinement rate reductions.
High-performance aligner materials: Multi-layer SmartTrack material has demonstrated up to 75% greater predictability compared to earlier single-layer aligner plastics, maintaining consistent force application throughout each wear cycle.
Precision bite ramps: For deep bite cases, precision bite ramps on upper incisors help manage the vertical dimension by disoccluding posterior teeth during anterior intrusion, though they should be viewed as part of a comprehensive strategy rather than a standalone solution.
9. Set Realistic Treatment Objectives
Perhaps the most important yet least technical strategy: set realistic goals. When treatment objectives exceed the biomechanical envelope of clear aligners, refinements become inevitable. Practicing orthodontists should consider:
• Defining treatment goals in writing — not just “straighten the teeth” but specific outcomes: Class I canine, 2mm overjet, 20% overbite, coincident midlines
• Matching the treatment modality to case complexity — complex extraction cases requiring significant root movement may benefit from sequential or hybrid fixed appliance therapy
• Documenting patient-specific risk factors (bone density, compliance concerns, periodontal status) and adjusting the plan accordingly
• Communicating realistic expectations to patients from the outset, including honest discussion of refinement probability for their specific case type
When Refinements Are Unavoidable: Recovery Strategies
Despite optimal planning and execution, some refinements remain unavoidable due to biological variation. When refinements are needed, the following strategies prevent them from becoming recurring cycles:
• Short recovery sequences vs. full refinements: Not every tracking issue requires a complete rescan. A targeted 3-5 tray recovery sequence can often resolve what would otherwise become a 20-tray refinement case.
• Make the first refinement the last: Invest the same planning rigor in refinements as in the original plan. Apply overcorrection, verify staging, and communicate precise clinical notes to the lab.
• Document and learn: Track which case types, movement types, and patient factors correlate with refinements in your practice. This data drives continuous improvement in case selection and planning protocols.